
This year I was given the opportunity to co-present a workshop at the 2014 OTA Victoria State Conference. As expected I launched at this opportunity with both hands! Having been involved with OTA QLD and the OTA National Conference before I was very keen to not only engage in some fantastic learning, but also to see how things are done/run in our south eastern quarter.
 photo credit: @nbalaa
photo credit: @nbalaa
The conference was held at the famous Flemington Racecourse and for this Queenslander the weather was quite crisp!
The formalities were kicked off by OTA CEO Rachel Norris who officially opened the conference.
Dr Rachael McDonald Keynote
Dr Rachael McDonald‘s keynote was one of my highlights of the entire conference. She talked about such a wide and varied number of topics and related them all back to the professions need to utilise our unique skill-set to promote the profession as a whole.

She spoke about the need for OT’s to embrace OCCUPATION as the utilisation of occupation is what sets us apart from other professions. She looked at the issue of OT’s promoting themselves from angles of working within restrictive policy environments, the current economic state of Australia and the fact that OT’s can often BE the barriers for our clients and used technology use as an example.
She referred to OT’s limiting their clients by filtering their interventions through their own values systems rather then basing it purely on the clients wishes.
Dr McDonald highlighted that OT’s have an exceptionally large “PR problem” and highlighted that with the NDIS being rolled out around the country that this inability to promote ourselves and what we do was only going to limit the work for the profession. She highlighted this as a major need to be part of Occupational Therapy Australia so they could have greater influence in saying “we are the peak body & here is why Occupational Therapy is really important.”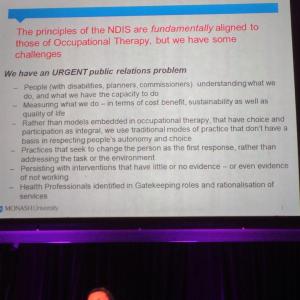 She pushed the message that “Occupation” was what we do, it is who we are, and it’s what we need to promote as our unique value in the health system. Dr McDonald made this very clear in saying, “We need to be able to clearly say: Here’s where you need an OT & here’s where someone else can do the job.”
She pushed the message that “Occupation” was what we do, it is who we are, and it’s what we need to promote as our unique value in the health system. Dr McDonald made this very clear in saying, “We need to be able to clearly say: Here’s where you need an OT & here’s where someone else can do the job.”
I left the Keynote feeling truly inspired that the range of projects I currently have on the go are all working in the right direction towards “selling” OT to the general public and unifying us as a profession.
Danielle Hitch - The current evidence base for mental health occupational therapy
Danielle Hitch’s first presentation was to bring to us her evaluation of the current evidence base for OT, that she did as part of her Phd. Danielle reported that she had reviewed 1700+ journal articles, pertaining to OT in mental health, which just seems unfathomable to me! The fact that there was even this much literature available regarding OT in mental health was a shock to a lot of the audience. She broke down the different topics and types of research and critiqued some of the general themes around types of research and how these were methods were actually recorded in the articles.

The biggest point I took out of this presentation is that there is a lot of work out there around OT’s in mental health and its not always published in the usual OT specific journals. I think this has encourage me to widen my search for evidence beyond my usual “go-to” sources.
Kate Andrews & Rebecca Hanrahan - introduction of an occupational therapy screening tool in acute mental health
This presentation was a clinical practice change project around introducing an occupation based screening tool that was consistent across 3(?) different acute units across the Alfred Health district.
The aim was to help promote a “united front” for the acute OT’s working in these wards. It would allow them to all be focusing on the same information. It would also allow for easy knowledge transfer between units and would cut down on number of repeat questioning by OT’s for consumers of the acute services. There were stipulated guidelines that stated that the completed screening tools would remain valid for 6 months and updated if appropriate. This would allow the OT’s to more efficiently screen consumers on admission to make the most efficient use of resources.
I was originally very interested in how this screen was implemented more then the actual screen itself as, having previously worked in an acute MH unit, I had also attempted to implement a screening process in a very different way then presented. The main issue identified was increased workload with the new tool, which aligned well with my own experience.
My practice change was about freeing up time to be able to complete occupational assessments with all consumers which would screen, assess and provide a starting point for Occ based intervention all in one. This project seemed to be more about using the time available more efficiently by hopefully cutting the number of inappropriate assessments through a brief screening process. In my reflecting about how this process might be implemented in my local acute unit it was clear that it wouldn’t be straight forward. The workload in the Alfred Acute MH wards is 1) spread across multiple units and 2) spread around multiple OT’s. This is not the case in the sole OT practitioner service of my local Acute Unit. I do however think that the time-frames for repeat assessment might be something for the current OT at my local Acute unit to consider with her Occupational Assessments.
The presenters were happy for their screening tool to be shared as long as it’s credited. Please find a copy of the Alfred Health Psychiatry Occupational Therapy Screening Tool as was provided during the presentation
 Alfred Health OT Screening Tool
Alfred Health OT Screening Tool
Janice McKeever- The evolution of occupational therapy practice in acute care settings: a scoping review
Janice presented a review of the scope of practice of OT’s in acute settings and examined how these might differ across countries. She found that in the literature the language used to describe the roles of OT’s in what is essentially similar roles paints a very different picture of the scope of practice and expectation of these roles. Janice emphasised the need to focus on occupation in these settings or risk being absorbed into the medical model health system. This type of review emphasised to me the role that culture and other contexts play in how we interpret our world and what we do within it. 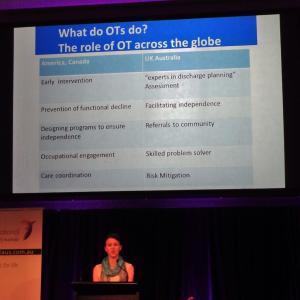
Associate Professor Natasha Lannin: Research in our practice - a requirement, not an option
Assoc Prof Natasha Lannin presented her Plenary session first up on day 2 of #otavic14. She explored some of the myths and barriers that surround why OT’s don’t get into research and adding to the evidence base of the profession.
 She stated that ALL occupational therapists needed to start writing up research and contributing to the spectrum of health evidence. She stated that it need only be small and that the vast majority of quality improvement projects that OTs regularly engage in could become “research” if a “little bit more rigour was added.”
She stated that ALL occupational therapists needed to start writing up research and contributing to the spectrum of health evidence. She stated that it need only be small and that the vast majority of quality improvement projects that OTs regularly engage in could become “research” if a “little bit more rigour was added.”
This being an area that I am gradually developing an ever growing interest it was fantastic to see the barriers to “research” being addressed in a practical way.
Aids & Equipment Alliance members: AT users and OTs - partners in finding technology solutions
Another one of my highlights of the conference was the amazing Natasha Layton with members of the Aids & Equipment Alliance presenting their Plenary session. It was amazing hear from people with lived experience the difficulties that services often put up due to a myriad of reasons that can often easily be avoided by simply talking to the consumer and working WITH them to make sure equipment and services actually meet their needs and don’t just tick service KPIs.
 The Alliance members gave profoundly insightful examples of things such as being able to touch the floor whilst in their wheelchair that may seem “functionally trivial” to most but then when they elaborated on the occupational barriers this simple oversight created it all of a sudden became a ‘not so trivial’ issue. By focusing on the occupational engagement with the assistance of technology and NOT the functional implications of using it our consumers are getting a better, more tailored service that will actually meet their needs….and it all starts with a simple conversation. I see many links between this example and other practice areas in OT, not just assistive technology!
The Alliance members gave profoundly insightful examples of things such as being able to touch the floor whilst in their wheelchair that may seem “functionally trivial” to most but then when they elaborated on the occupational barriers this simple oversight created it all of a sudden became a ‘not so trivial’ issue. By focusing on the occupational engagement with the assistance of technology and NOT the functional implications of using it our consumers are getting a better, more tailored service that will actually meet their needs….and it all starts with a simple conversation. I see many links between this example and other practice areas in OT, not just assistive technology!
for more info please visit: aeaa.org.au
Kathryn Legg - The value of an occupation-based martial arts as therapy program for children who have a parent with a mental illness
Kathryn presented her research project that was an OBP Martial arts program for children with family who have a mental illness.
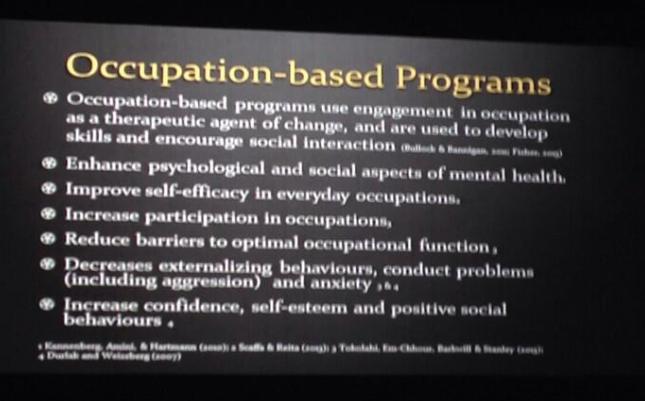
The main points I took from this presentation were not that the children engaged in the occupation of martial arts (which is awesome in it’s own right!) but the flow-on effects into their lives outside of these classes. Skills that they learned and translated from the occupation of martial arts such as anger management and relaxation, organisation and increase in self care. These, to me, really highlighted the amazing, powerful and complex nature of occupation as a therapeutic tool. I’ve seen very few tools more powerful then Occupation as Means!
Reclaiming Occupation as Means (ROAM): Creating communities of occupation-centred occupational therapists
So my fellow ROAMen, James Naismith and Dr Robert Pereira were given the honour of presenting the one and only workshop at #OTAVIC14. We wanted to present the ROAM project that we had been working on collectively in a way that would demonstrate the timely need for such a project.
The main thing I recognised in running this workshop was the atmosphere. I’m normally quite comfortable in public speaking and I didn’t feel particularly uncomfortable with this gig but there was a “vibe” in the room that I initially couldn’t put my finger on. It was different to any other workshop or talk I’ve ever done.
On reflection there are a couple things that I feel may have contributed to this. Firstly, the sheer size of the room. I’m used to speaking quite naturally and usually don’t use a microphone but in a room that could easily facilitate 400 people your voice would be lost amongst the space so a microphone was a necessity. The second thing I noticed is that the demographic of the audience was very different to other events that I’ve spoken at. I estimate that crowd was over 50% upper management and academic OT’s which was interesting as that’s a demographic I’ve not previously had much buy-in from when I’ve done similar talks on similar topics and so hence the content and my presenting style was possibly more tailored to coalface clinicians. I’m still extremely happy with how the workshop happened and the discussions stimulate were very valuable. I think it was excellent for me to be put slightly out of my comfort zone, to show me that there are still things that I need to be conscious of when presenting to new audiences.
Content wise I think some of the discussions highlighted the mixed perspectives on OBP that are littered throughout our professions. There were managers who were really pushing OBP in their districts, clinicians who looks puzzled, lecturers who couldn’t understand that why this wasn’t “being done in practice when we’re teaching it?”
Overall for myself it highlighted the need to have these discussions across the profession as lots of facets of OT have their own perspective on the place of OBP in OT and if/how its being implemented.
This cemented, to me, the need for ROAM!
Ms Kate MacRae Keynote
Kate MacRaes Keynote was around the practical functioning of a health service and a project that she ran that I wish EVERY health service could replicate. She started by mapping a clients journey through the health service after a fractured neck of femur. She found that the the client had gone through 5 different services, which meant 5 intake assessments, 5 intake meetings, 5 waiting lists, 5 service provisions, 5 referrals and a total of 34 different clinicians not including nursing staff during inpatient stays.
Her project took a team of people and put them in a room to redesign the health service from scratch! Ignoring all previous preconceptions and internal requirements/team structures. A blank slate to create a service that would better and more efficiently meet their clients needs. She used two videos in her presentation that I found exceptionally powerful. Firstly to really explain empathy compared to what is commonly experienced by clients using a health system. The second is a powerful video that really highlights the unbelievable power of context, and specifically the client narrative in delivering health care.
Social Media at #OTAVic14
One thing that I was really happy to see was the push for social media engagement during the conference. The conference committee was aware of the benefits of promoting the conference across multiple platforms. The hashtag and SocMe platforms was well promoted around the venue with signs such as the one below highlighting the platforms, the links to the association on those platforms, QR codes that link to the association on those platforms and the conference hashtag attendees were able to utilise. The hashtag was also a feature on all generic and introduction slides during the presentation sessions which is something I’d most definitely recommend other divisions look into doing.
 The hashtag attracted interest from all over the world from OT’s interested and asking questions about the presenters and happenings at the conference. The ability for the association to engage with its members and attendees across multiple platforms was amazing to watch and experience! Bravo to the OTA Vic conference committee in promoting modern technology engagement!
The hashtag attracted interest from all over the world from OT’s interested and asking questions about the presenters and happenings at the conference. The ability for the association to engage with its members and attendees across multiple platforms was amazing to watch and experience! Bravo to the OTA Vic conference committee in promoting modern technology engagement!
Overall I had a fantastic time at OTA Vic Div Conference and would definitely recommend it to any OT 🙂
Note: for an excellent summary of all the Twitter activity from #otavic14 check out Anita Hamilton‘s Storify: https://storify.com/VirtualOT/otavic-state-conference-may3-4-2014