Last weekend I attended the 2013 Mental Health & Paediatric Symposia at Seaworld on the Gold Coast.
This was a fantastic event which, (I’ve heard) had a few hiccups behind the scenes but ran seamlessly for attending delegates.

The symposium format (longer workshops rather then short rapid fire presentations) allowed time for the processing of new ideas and concepts and the discussion of these. I felt like this allowed me to learn a lot more ‘whole concepts’ rather then initial introductions to many different topics.
I was honored to also be invited to speak on the professional use of technology and apps in occupational therapy.
Tina Champagne Keynote: Reclaiming Occupation: A Non Linear Science Approach
DISCLAIMER: This was a VERY complex and heavy concept but I’ll reflect upon my understanding of it. I may be completely wrong but this is my subjective experience.
I’ve been quite keen to hear this keynote for some time. For a long while in my discussions with her Tina has mentioned this “Non-Linear Science” but I’d never understood exactly what she was talking about, so when she told me she was going to give her keynote on the topic I was very keen to soak this in.
I’d be lying if i didn’t get a little satisfaction seeing Tina used one of my Occupational Musings as a slide in her presentation to highlight Matthew Molineux’s “Nature of Occupation”. (Molineux, 2010) 
Tina started by explaining that the theories of non-linear science evolved from mathematics and physics and other “sciences” that delt with non-linear dynamic systems. It is also easily recognized that the Human body and life itself is also a non-linear dynamic system. This view of human beings is an interesting one that on the whole seems to sit outside any health specific models. Most of the points made absolute subjective sense to me whilst sitting there. My experiences with life, people, injury, the environment all seemed to fit quite easily within this idea that all things are codependent on each other. There seemed to be something very ‘spiritual’ about this way of thinking. The fact that there was a connection, an influence, a correlation between every “system” and its environment. And the fact that the influence is a two way dynamic. The system influences the environment and the environment influences the system. Now I know that OT’s are reading this and going….”deeeerrrr.” But the point that this brings up is that OT’s are always looking at the evidence behind something (or lack of). Non-linear science takes already well established scientific theories such as Chaos Theory and shows how humans as occupational beings can be explained/fit into this (in this example) well researched astrophysics theory. 
The concept that a human being is a self-organising, non-linear dynamic system may sound very complicated but in essence its something that most of us have always known. Its just being described using a scientific language common across many professions the world over. This idea that what we have been doing for years can already be explained by seemingly unrelated science that was established many many many years prior to our profession even beginning did initially make me skeptical. But everything that was presented made perfect sense to me. It’s an extremely large and complex field of theory but I’ve committed to have a look into it.
The comparison between a Classical Science and a Nonlinear Science was a really good demonstration of the correlation to how Occupation fits better within it then a traditional science lens.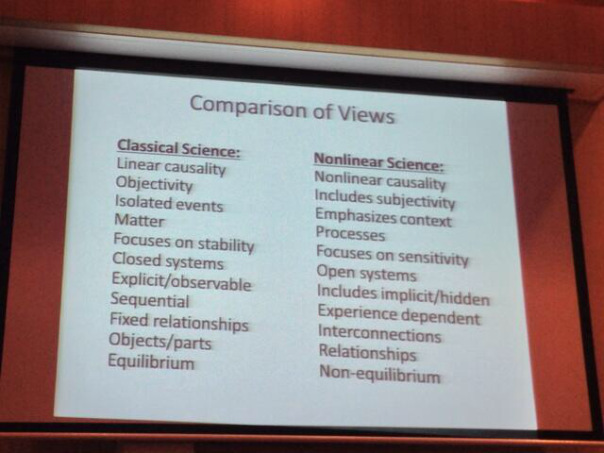
Overall it was an extremely interesting perspective on occupation and Occupational Therapy that I had not previously been exposed to. It’s definitely something that I want to read up more on and will be continuing discussions with Tina about this in the future.
and of course I couldn’t let her get away without a shameless fan pic 
Embracing New Technologies in Occupational Therapy: from Social Media to Apps
With the social media aspect I took a different approach to previous presentations in that, previously I spent a lot of time looking at what exactly makes up the power of social media and the different types of user categories. This presentation I wanted it to be a little more”hands on”. I still have a very brief talk on the sheer size of some of hue he major social media tools (Facebook & Twitter) to highlight why we use them. Then I went right into examples of professional social media use as well as how these experiences can be utilised towards a clinicians CPD record.
OTA QLD Mental Health and Paediatric Symposia 2013 from Brock Cook

Adam showed some Apps that he had found (can be seen in the embedded presentation) One thing that Adam presented on that really caught my eye was Massive Online Open Courses (MOOC).
It is a free web based platform that allows the user to develop and implement online training courses. It is currently be used by various universities from all around the world. This is something that I believe I may be able to utilize in the future and one that I will be thoroughly exploring!
Occupation Based Practice: It’s time to walk the talk
The first thing I hear from Matthew as I walk into the room is “why are you in here? You’ve heard this a thousand times” This statement along got me thinking, before the workshop had even started. Yes I had heard quite a few talks on Occupation Based Practice, and yes I had seen/heard Matthew give quite a few of those. So what was I there?
I have a firm belief that I’m still in a very novice stage of my knowledge about Occupation Based Practice. Maybe comparatively not but that is where I subjectively rate myself to be sitting at this time. So one reason I was there was because every time I listen to a talk on OBP I absorb something different. A reference. A concept. An Idea. A view. Whatever it is i get a little something different each time which I add to my overall bolus of knowledge. Slowly growing it bigger.
One way that I think this happens is that each of the talks has different participants, working in different settings, in different places. All of these contextual factors mean that different examples, questions and confusions arise in each different talk. These are where I learn to apply some of my acquired knowledge to various contexts to see how i might view the situation if placed in that other persons shoes. I guess I’m grounding my knowledge.
This particular talk caught my eye with the title.
“Occupation Based Practice: It’s time to walk the talk”
This seemed to fit perfectly with where I am at in my professional reform journey. I have quite a lot of the basic theoretical knowledge behind me now. I’m comfortable talking about Occupation and OBP and now am in the process of trialing different methods of operating in my workplace.

Some interesting concepts came up that I hadn’t thought of before. One was the different categories of practice. Direct Service Provision, Indirect Service Provision and Consultancy. Obviously the ideal situation is to be providing OBP by direct service provision. That is pure beautiful occupational therapy. In my current role however I feel that with the environmental restrictions due to the ward and the Mental Health Act quite often what I do would fit within Indirect Service Provision. I may well sit and do all the groundwork with a consumer but then organise with Community teams or NGO’s to actually assist the consumer in engaging in the occupations they they identified as meaningful to them.
This on its own raised some important questions.
I’m already of the opinion that the AMHU may not be a setting where OT is ideally placed, and looking at it from this point of view kind of validated this feeling in a way. But it also raised more questions.
- Is it ok to fall solely into an indirect service provision role?
- What are the outcome difference between direct and indirect service provision if the consumer is engaging in their occupations with both?
- Should I be fighting the system to include more Direct OBP Service Provision in my workplace?
All these questions have highlighted new gas in my knowledge that I feel an innate need to have answered before I am able to proceed in re-engineering my current role.
Whatever the answers may be, the truth is that there has been enough talk and it’s time to be occupation based.
How to be wanted when your are not wanted: Engaging disengaged consumers
On the second day I attended a Mental health panel discussion about techniques and examples of how to engage with consumers who are disengaged with the service.
The panel of 6 OTs from various MH practice areas each gave an example or two of a time when they were able to engage with a difficult or disengaged client. These “techniques” were then collated in a list on a whiteboard for everyone’s reviewing.
Throughout the 19 or so techniques that ended up being listed I drew two very simple conclusions/techniques.
1) the client needs to be given back the locust of control of the situation. It’s no use in trying to force rapid rapport building on a person as all the most amazing communication techniques in the world won’t make it work if the consumer is feeling pressured and doesn’t want to engage in the first place.
So I suggested to the group that the key is to simply let the consumer have complete control of the process. Make herself and what you offer available and if they want it, they’ll come to you.
2) please don’t lie to your consumers for the purpose of speeding up the rapport building process. This is a sure fire way to kill any rapport you have managed to build in an instant.’
Taking the rapport building process slow and engaging in occupations with the consumer is by far the best and most effective method of engaging disengaged consumers I’ve ever used.
Overall I had a fantastic experience at the OTA QLD Mental Health & Paediatric Symposium, catching up with old friends, making new friends and learning new things. I’ll definitely be looking forward to this type of even again in the future.
